CHAMBER ENLARGEMENT AND HYPERTROPHY
OVERVIEW
- WHAT IS CHAMBER ENLARGEMENT?
- WHAT IS HYPERTROPHY?
- RIGHT ATRIAL ENLARGEMENT
- LEFT ATRIAL ENLARGEMENT
- RIGHT VENTRICULAR HYPERTROPHY
- LEFT VENTRICULAR HYPERTROPHY
- WHAT IS CHAMBER ENLARGEMENT AND HYPERTROPHY?
CHAMBER ENLARGEMENT– Increase in size of atria/ventricle. no muscle thickness present. It can affect both atria.
HYPERTROPHY– Is thickening of the wall of the chamber. This thickening may result in elevation of pressure within the heart and sometimes poor pumping action. The most common cause is high blood pressure. It mainly affect ventricles.
RIGHT ATRIAL ENLARGEMENT
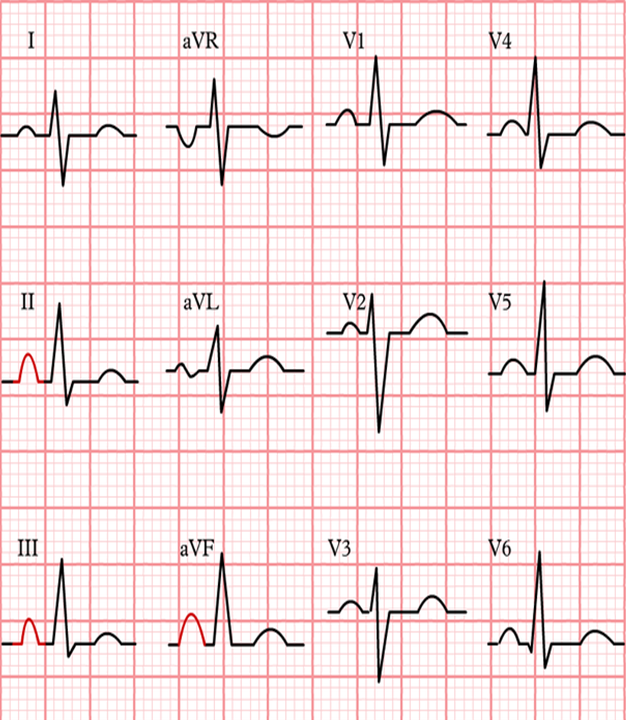
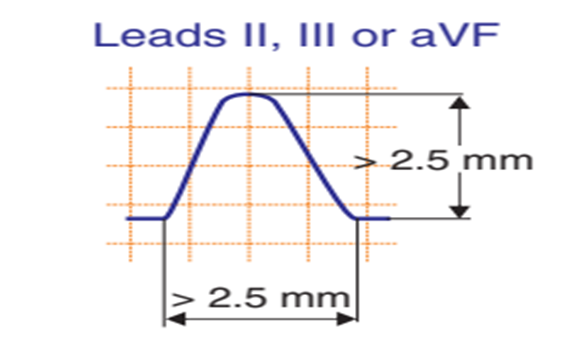
- Right atrial enlargement is defined as either:-
- P >2.5 mm in II / III and / or aVF.
- P >1.5 mm in V1.
- Right atrial enlargement can result from increased pressure in the pulmonary artery, e.g. after pulmonary embolization. A positive part of the biphasic p-wave in lead V1 larger than the negative part indicates right atrial enlargement. The width of the p wave does not change.
LEFT ATRIAL ENLARGEMENT
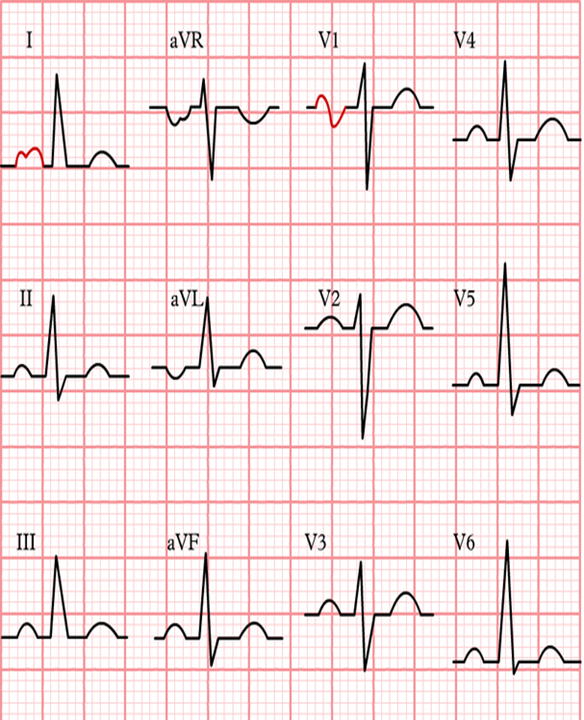
- Criteria for left atrial enlargement. Either
- P wave with a broad (>0.04 sec or 1 small square) and deeply negative (>1 mm) terminal part in V1
- P wave duration >0.12 sec in leads I and / or II
- Left atrial enlargement is often seen in mitral valve insufficiency, resulting in back flow of blood from the left ventricle to the left atrium and subsequent increased local pressure.
BIATRIAL ENLARGEMENT
- Biphasic P wave in V1 of more than 0.04 sec duration. The positive initial part is > 1.5mm and the negative terminal part > 1mm
- In biatrial enlargement the ECG shows signs of both left and right atrial enlargement. In V1 the P wave has large peaks first in a positive and later in a negative direction.
RIGHT VENTRICULAR HYPERTROPHY
- Right ventricular hypertrophy occurs mainly in lung disease or in congenital heart disease. The ECG shows a negative QRS complex in I (and thus a right heart axis) and a positive QRS complex in V1.
- QRS duration < 120ms Right heart axis deviation (> 110 degrees)
- Dominant R wave:
- R/S ratio in V1 or V3R > 1, or R/S ratio in V5 or V6 <= 1 R wave in V1 >= 7 mm
- R wave in V1 + S wave in V5 or V6 > 10.5 mm
- rSR= in V1 with R’= > 10 mm
- qR complex in V1.
- Secondary ST-T changes in right precordial leads
- Right atrial abnormality
- Onset of intrinsicoid deflection in V1 between 0.035 and 0.055sec.
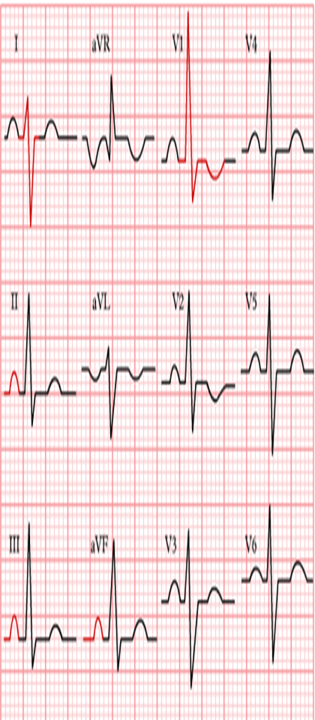
LEFT VENTRICULAR HYPERTROPHY

- Commonly used ECG criteria for diagnosis of LVH :
- S in V1 + R in V5 or V6 (whichever is larger) ≥ 35 mm (or 3.5 mV)
- R in aVL ≥ 11 mm or if left axis deviation R in aVL ≥ 13 mm plus S in III ≥ 15 mm
- R in I + S in III > 25 mm
- Delayed intrinsicoid deflection in V6 ≥ 50 ms.
- The ECG criteria for diagnosing LVH are very insensitive (about 20–50%) meaning that many patients with LVH cannot be recognized by ECG (false negatives!). However, the criteria are very specific (about 90%) which means it is very likely that LVH is present if the criteria are met.
CAUSES OF HYPERTROPHY
CAUSES OF RVH
-Heart Failure
-Chronic Obstructive Pulmonary Disease
-Pulmonary Embolism.
-Atrial Septal Defect (A Hole In The Wall Between Your Heart’s Upper Chambers)
-Pulmonary Valve Stenosis
-Tricuspid Valve Regurgitation
-Tetralogy Of Fallot
-Ventricular Septal Defect (A Hole In The Wall Between Your Heart’s Lower Chambers)
CAUSES OF LVH
-High blood pressure (hypertension)
-Aortic valve stenosis
-Athletic training
-Hypertrophic cardiomyopathy. This genetic disease occurs when the heart muscle becomes abnormally thick, even with completely normal blood pressure, making it harder for the heart to pump blood.
-Amyloidosis. A condition that causes abnormal protein deposits around the organs, including the heart.